GABAPENTIN SCHEDULING AS A CONTROLLED SUBSTANCE: A GUIDE TO PDMP REPORTING LAWS IN THE US
Gabapentin, initially developed as a treatment for epilepsy, has gained widespread use for managing various types of pain. In recent years, it has received significant attention, largely due to concerns about the drug’s abuse and misuse. As a result, several states have rescheduled gabapentin to control its availability and limit its potential for harm. Healthcare providers must be vigilant when prescribing and dispensing the medication. This post aims to offer guidance to healthcare providers involved in prescribing and dispensing gabapentin.

- Gabapentin Products
- Gabapentin Mechanism of Action
- Gabapentin FDA-Approved Indications and Off-Label Uses
- Patients Most at Risk of Gabapentin Abuse and Misuse
- How Gabapentin is Abused and Misused
- Gabapentin Adverse Reactions
- States Where Gabapentin is a Schedule 5 Controlled Substance
- States that Have Mandated Gabapentin Reporting to PMPs
- States that are Deliberating Whether to Add Gabapentin as a Controlled Substance or to their Mandated Reporting Programs
- References
Products
Gabapentin is sold under the following brand names (not all inclusive):
- Active-PAC with gabapentin: oral capsule;
- Gralise: oral tablet, ER;
- Horizant: oral tablet, ER; and
- Neurontin: oral capsule, tablet, solution
Mechanism of Action
The analgesic mechanism of gabapentin remains unknown, but it has been shown to prevent allodynia and hyperalgesia in animal models of neuropathic pain. Gabapentin has also exhibited anticonvulsant activity in preclinical models, although its relevance to human epilepsy is unclear. While structurally related to the neurotransmitter GABA, gabapentin does not bind to common receptor sites and does not modify GABA uptake or degradation. Although a gabapentin binding site has been identified in certain areas of the brain, its functional significance remains to be determined1.
FDA-Approved Indications and Off-label Uses
Gabapentin is currently FDA-approved for use in postherpetic neuralgia and particular seizure disorders2. However, it is frequently used for the following off-label uses3,4,5:
- Sleep disorders.
- Anxiety
- Sciatic back pain.
- Diabetic neuropathy.
- Fibromyalgia.
- Headaches
- Migraine prophylaxis.
- Restless leg syndrome.
- Perimenopausal hot flashes.
- Mood disorders.
- PTSD.
Patients Most at Risk of Abuse and Misuse
Patients most at risk of gabapentin abuse and misuse are those with a history of or current substance misuse/abuse/dependence, particularly opioid misuse6. Studies of opioid abuse samples in the US and UK estimated gabapentin misuse to be between 15-22%7,8,9, and gabapentin abuse with a prescription ranged from 40-65%8,9,10,11. There is little evidence of gabapentin abuse among those with a positive history of alcohol abuse or dependence6,12.
How Gabapentin is Abused and Misused
Gabapentin is frequently combined with other substances for the purpose of potentiating the effects of the drugs or achieving a “high.” Studies have identified various substances that are commonly abused in combination with gabapentin, including alcohol, opioids, benzodiazepines, antidepressants, and other CNS depressants13,14,15. Individuals who misuse gabapentin are also more likely to misuse prescription opioids and benzodiazepines8. Reported combinations of gabapentin abuse include buprenorphine, methadone, ethanol, cannabis, SSRIs, LSD, amphetamine, and GHB16.
Adverse Reactions
Gabapentin has been observed to potentially induce unfavorable side effects in some individuals. Healthcare providers should regularly evaluate for and encourage patient reporting of side effects. If taken in higher than recommended dosages or combined with other substances, the side effects may become more severe. For example, when used concurrently with opioid medications, gabapentin has been linked to increased risk of severe adverse effects, including fatality17.
Most common adverse reactions2:
- Dizziness
- Somnolence
- Peripheral edema
- Ataxia
- Fatigue
- Nystagmus
- Viral infection
- Fever
- Nausea and/or vomiting
- Hostility
Less common, serious adverse reactions2:
- Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS)/Multiorgan Hypersensitivity
- Anaphylaxis and Angioedema
- Withdrawal Precipitated Seizure
- Status Epilepticus
- Suicidal Behavior and Ideation
- Neuropsychiatric Adverse Reactions (Pediatric Patients 3 to 12 Years of Age)
- Sudden and Unexplained Death in Patients with Epilepsy
Compliance with State and Federal Gabapentin Reporting Regulations
Gabapentin is not currently listed as a controlled substance under federal law. However, some states classify gabapentin as a Schedule V substance or a drug of concern and mandate reporting to PMP. Furthermore, other states are considering similar actions due to increasing evidence of associated risks. This has made prescribing and dispensing gabapentin complex, particularly across state borders. A discussion of the reporting requirements per state is provided below.
Please note- the following terms are used interchangeably below: gabapentin, controlled substance(s), and covered substance(s).
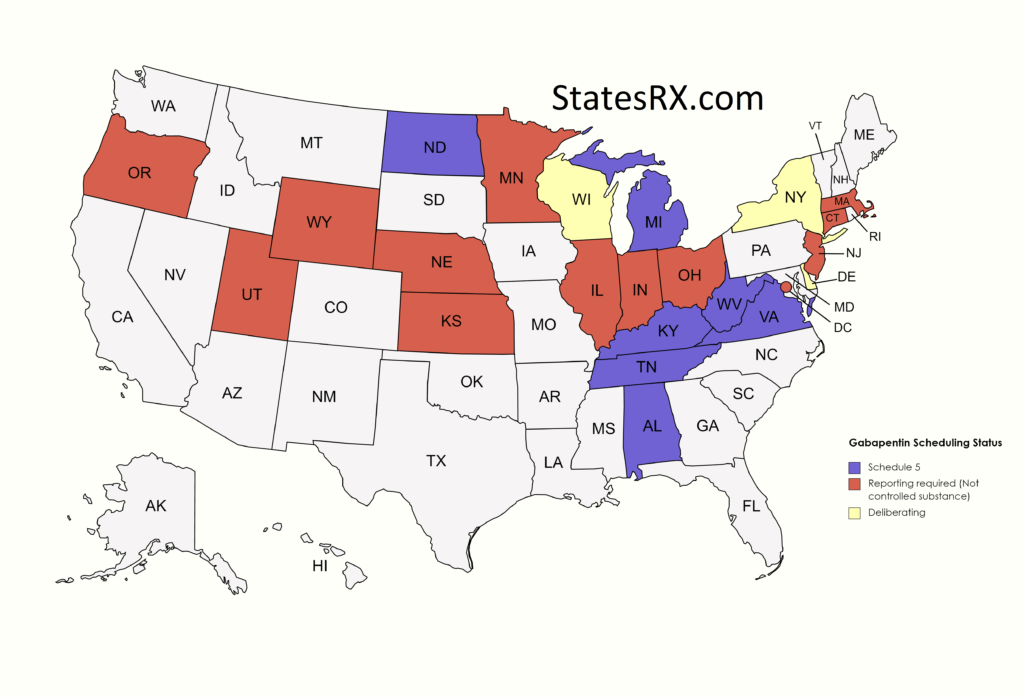
States where gabapentin is a schedule V controlled substance, As of April 2023:
- Alabama (AL)
- Reporting38:
- The following entities or practitioners are subject to the reporting requirements:
- Licensed pharmacies, not listed under the Exemptions section below.
- Mail order pharmacies or pharmacy benefit programs filling prescriptions for or dispensing gabapentin to residents of this state.
- Licensed physicians, dentists, podiatrists, or optometrists who dispense gabapentin directly to patients.
- Exemptions:
- Pharmacies of general and specialized hospitals, nursing homes, and any other health care facilities which provide inpatient care, so long as gabapentin is administered and used by a patient on the premises of the facility.
- Sample medications.
- Gabapentin administered to patients during the course of treatment is excluded from the reporting requirement
- The following entities or practitioners are subject to the reporting requirements:
- Reporting38:
- Kentucky (KY)
- Reporting 39:
- The data shall be transmitted to KASPER no later than close of business on the business day immediately following the dispensing unless the cabinet grants an extension.
- Exemptions 40:
- A drug administered directly to a patient in a hospital, a resident of a health care facility, a resident of a child-caring facility, an individual in a jail, correctional facility or juvenile detention facility.
- The quantity dispensed is limited to an amount adequate to treat the patient for a maximum of 48 hours.
- Reporting 39:
- Michigan (MI)
- Reporting 41:
- All pharmacies, dispensing practitioners, and veterinarians who dispense gabapentin are required to electronically report this prescription data to MAPS on a daily basis. The data required shall be forwarded to the department by the end of the next business day and shall include data for all controlled substances dispensed since the previous transmission or report.
- Exemptions:
- Reporting exemptions include gabapentin administered to patients.
- Samples of gabapentin provided to a patient.
- Gabapentin dispensed by a physician at a medical institution for a maximum of 48 hours.
- Reporting 41:
- North Dakota (ND)
- Reporting 42:
- Each dispenser shall submit to the board by electronic means information regarding each prescription dispensed for a controlled substance.
- Exemptions:
- Does not include a licensed hospital pharmacy that provides gabapentin for the purpose of inpatient hospital care
- A licensed health care practitioner or other authorized individual in those instances when the practitioner administers gabapentin directly to a patient.
- Reporting 42:
- Tennessee (TN)
- Reporting43:
- Any pharmacy, or licensed healthcare practitioner, who has a DEA number and dispenses gabapentin in (or into) Tennessee must report to the database daily (but no later than the close of business on the following business day) each controlled substance they have dispensed over the last 24 hours.
- Veterinarians are only required to submit prescriptions every 14 days.
- Exemptions:
- Gabapentin prescribed for administration directly to a patient during the course of inpatient or residential treatment in a hospital or nursing home or during the course of inpatient treatment in a hospital licensed under title 33.
- The drug is a sample that is provided to the patient without charge. In order to be exempt from reporting, a sample of gabapentin must be in a quantity limited to an amount that is adequate to treat a patient for a maximum of 14 days.
- The drug is dispensed by a licensed veterinarian and in a quantity limited to an amount that is adequate to treat the non-human patient for a maximum of 5 days.
- Reporting43:
- Virginia (VA)
- Reporting44:
- Gabapentin must be reported within 24 hours or the dispenser’s next business day. The program also requires non-resident pharmacies to report dispensing of gabapentin to Virginia residents.
- Reporting44:
- Exemptions45:
- Dispensing of manufacturers’ samples of gabapentin or of gabapentin dispensed pursuant to an indigent patient program offered by a pharmaceutical manufacturer.
- Dispensing of gabapentin by a practitioner of the healing arts to his patient in a bona fide medical emergency or when pharmaceutical services are not available.
- Administering of gabapentin.
- Dispensing of covered substances within an appropriately licensed narcotic maintenance treatment program.
- Dispensing of covered substances to inpatients in hospitals or nursing facilities licensed by the Board of Health or facilities that are otherwise authorized by law to operate as hospitals or nursing homes in the Commonwealth.
- Dispensing of gabapentin to inpatients in hospices licensed by the Board of Health.
- Dispensing of covered substances by veterinarians to animals within the usual course of their professional practice for a course of treatment to last 7 days or less or if such covered substance is feline buprenorphine or canine butorphanol.
- Exemptions45:
- West Virginia (WV)
- Reporting46:
- Every pharmacy (including out-of-state pharmacies) that services outpatients and dispenses gabapentin is required to submit the dispensing information to the WVBOP.
- Reporting is for a drug dispensed to a patient by a practitioner: Provided that the quantity dispensed may not exceed an amount adequate to treat the patient for a maximum of 72 hours with no greater than two 72-hour cycles dispensed in any 15-day period of time.
- Reports must be submitted no later than 24 hours after dispensing.
- Exemptions:
- A drug administered directly to a patient by a practitioner.
- Reporting46:
States that have mandated gabapentin reporting to their PMPs, AS OF APRIL 2023:
- Connecticut (CT)
- Reporting18:
- Dispensation information is required to be uploaded into the CPMRS if prescribed for more than a 48-hour supply.
- Exemptions:
- If administered directly to a patient by a prescriber.
- If drug sample is dispensed.
- If dispensed to inpatients in hospitals or nursing homes.
- If dispensed to inpatients in hospices.
- If dispensed by any facility that is registered by the U.S. DEA as a narcotic treatment program.
- Reporting18:
- District of Columbia (Washington DC)
- Reporting19:
- Each dispenser of a covered substance shall submit the prescription monitoring data required to the Program within 24 hours after a covered substance is dispensed for each covered substance dispensed.
- Exemptions:
- Administering gabapentin.
- Dispensing gabapentin within an appropriately licensed narcotic maintenance program, such as a methadone treatment program or substance abuse treatment program.
- Dispensing gabapentin to inpatients in hospitals or nursing facilities licensed by the Department or facilities that are otherwise authorized by law to operate as hospitals or nursing homes in the District.
- Dispensing gabapentin to inpatients in hospices licensed or certified by the Department.
- Reporting19:
- Indiana (IN)
- Reporting20,21:
- Each time gabapentin is dispensed, the dispenser is required to transmit specific information to INSPECT.
- Licensed dispensers throughout Indiana—and out-of-state (non-resident) pharmacies licensed to dispense drugs in Indiana—are required to submit prescription data to INSPECT every 24 hours.
- Exemptions:
- The requirement does not apply when a drug is administered directly to the patient.
- The requirement does not apply when a drug is dispensed by a practitioner, if the quantity dispensed is not more than a 72-hour supply.
- Reporting20,21:
- Kansas (KS)
- Reporting 22,23:
- Each dispenser (pharmacy) is required to electronically submit information to K-TRACS within 24 hours of each gabapentin prescription dispensed in an outpatient setting.
- If a prescriber or a pharmacist has a concern about a patient, he/she can look up the patient’s prescription history in K-TRACS.
- Exemptions:
- The only exception is for quantities dispensed in the emergency room for 48 hours or less.
- Reporting 22,23:
- Massachusetts (MA)
- Reporting 24,25:
- The reporting requirement shall apply to every pharmacy that dispenses gabapentin, and to any pharmacy in another state, commonwealth, district or territory that delivers such drug to a person in Massachusetts.
- The information required shall be transmitted by the end of the next business day.
- Exemptions:
- This requirement shall not apply to the dispensing of gabapentin to an inpatient in a hospital.
- Reporting 24,25:
- Minnesota (MN)
- Reporting 26,27:
- Dispensers are required to report on a daily basis (same day or next business day.)
- Exemptions:
- When a drug is distributed through the use of an automated drug distribution system.
- A dispenser is not required to submit this data for individuals receiving a drug sample that was packaged by a manufacturer and provided to the dispenser for dispensing as a professional sample.
- A dispenser is not required to submit this data if an Opioid Treatment Program pharmacy or facility is unable to report due to data privacy measures in Federal Regulations 42 CFR part 2.
- Licensed hospital pharmacy that distributes gabapentin for inpatient hospital care only is not required to submit this data.
- Reporting 26,27:
- Nebraska (NE)
- Reporting 28,29:
- Dispensers are required to electronically report data on gabapentin prescriptions dispensed to a patient (human) in Nebraska or to an address in the state.
- Dispensers are required to submit data at least daily in a standardized format.
- Exemptions:
- The delivery of gabapentin for immediate use for purposes of inpatient hospital care or emergency department care.
- The administration of gabapentin by an authorized person upon the lawful order of a prescriber.
- A wholesale distributor of gabapentin monitored by the prescription drug monitoring system.
- The dispensing to a nonhuman patient of gabapentin.
- Reporting 28,29:
- New Jersey (NJ)
- Prescriber actions 30:
- A pharmacy filling a prescription for gabapentin in an outpatient setting, shall collect and electronically transmit to the Division’s PMP vendor on a daily basis information for each prescription.
- Exemptions:
- The direct administration of gabapentin to the body of an ultimate user;
- The reporting requirements shall not apply to any prescriptions filled by a pharmacy for gabapentin dispensed to an inpatient at a hospital, long-term care, or other facility in which the resident is provided with 24-hour nursing care.
- Prescriber actions 30:
- Ohio (OH)
- Reporting 31,32:
- All pharmacies located outside this state and licensed as a terminal distributor of dangerous drugs that dispense gabapentin to outpatients residing in this state.
- All pharmacies located within this state and licensed as a terminal distributor of dangerous drugs that dispense gabapentin to all outpatients.
- All wholesalers licensed as a wholesale distributor of dangerous drugs that sell gabapentin at wholesale shall report those drug transactions.
- All pharmacies licensed as a terminal distributor of dangerous drugs that sell gabapentin at wholesale shall report those drug transactions.
- All prescribers, except veterinarians, located within this state that personally furnish gabapentin to outpatients, including samples.
- Exemptions:
- Products administered to a patient while in the office (such as an injection) do not need to be reported.
- Reporting 31,32:
- Oregon (OR)
- Reporting33:
- Dispensers are required to report dispensations of gabapentin to the OR PDMP within 72 hours after the drug is dispensed.
- Exemptions47:
- Institutional pharmacies as designated in ORS 179.321 including, but not
- limited to, those within the Department of Corrections, Oregon State Hospital Campuses, and Eastern Oregon Training Center as defined in 179.10 and 421.005.
- If administered directly to a patient as or pursuant to ORS 127.800 (Death with Dignity Act).
- Manufacturing and wholesale drug outlets servicing retail and inpatient
- Veterinary pharmacies are exempt from reporting per statute.
- Reporting33:
- Utah (UT)
- Reporting34,35:
- Each pharmacy or pharmacy group shall submit the data required on a daily basis, either in real time or daily batch file reporting. The submitted data shall be from the point-of-sale date.
- Reporting34,35:
- Wyoming (WY)
- Reporting36:
- Resident and nonresident retail pharmacies shall ensure that, not later than the close of business on the business day immediately following the day the gabapentin was dispensed, the information required is transmitted.
- Exemptions:
- An inpatient of a hospital, correctional institution or nursing facility.
- Reporting36:
- Illinois (IL)
- Reporting37:
- The information required must be transmitted not later than the end of the business day on which gabapentin is dispensed, or at such other time as may be required by the Department by administrative rule.
- Exemptions:
- A licensed veterinarian is exempt from the reporting requirements of this Section.
- Reporting37:
States that are deliberating whether to add gabapentin as a controlled substance or to their mandated reporting programs, AS OF APRIL 2023:
- Delaware (DE)
- New York (NY)
- Wisconsin (WI)
References
- Gee NS, Brown JP, Dissanayake VUK, Offord J, Thurlow R, Woodruff GN. The novel anticonvulsant drug, gabapentin (Neurontin), binds to the α2δ subunit of a calcium channel. Journal of Biological Chemistry. 1996;271(10):5768-5776.
- S. Food and Drug Administration. (2020). Neurontin (gabapentin) capsules, tablets, and oral solution. Retrieved from https://www.accessdata.fda.gov/drugsatfda_docs/label/2009/020235s041,020882s028,021129s027lbl.pdf
- Peckham, A.M., Evoy, K.E., Ochs, L., & Covvey, J.R. (2018). Gabapentin for off-label use: Evidence-based or cause for concern? Substance Abuse, 12, 1-8.
- Macdonald KJ, Young LT. Newer antiepileptic drugs in bipolar disorder: rationale for use and role in therapy. CNS Drugs. 2002;16:549–562.
- Mack A. Examination of the evidence for off-label use of gabapentin. J Manag Care Pharm. 2003;9:559–568.
- Smith RV, Havens JR, Walsh SL. Gabapentin misuse, abuse and diversion: a systematic review: Gabapentin misuse and diversion review. Addiction. 2016;111(7):1160-1174.
- Baird CR, Fox P, Colvin LA. Gabapentinoid abuse in order to potentiate the effect of methadone: a survey among substance misusers. European addiction research. 2014;20:115–118.
- Smith RV, Lofwall MR, Havens JR. Abuse and diversion of gabapentin among nonmedical prescription opioid users in Appalachian Kentucky. The American journal of psychiatry. 2015;172:487–488.
- Wilens T, Zulauf C, Ryland D, Carrellas N, Catalina-Wellington I. Prescription medication misuse among opioid dependent patients seeking inpatient detoxification. The American journal on addictions/American Academy of Psychiatrists in Alcoholism and Addictions. 2015;24:173–177
- Kapil V, Green JL, Le Lait MC, Wood DM, Dargan PI. Misuse of the gamma-aminobutyric acid analogues baclofen, gabapentin and pregabalin in the UK. British journal of clinical pharmacology. 2014;78:190–191.
- Klein-Schwartz W, Shepherd JG, Gorman S, Dahl B. Characterization of gabapentin overdose using a poison center case series. Journal of toxicology Clinical toxicology. 2003;41:11–15.
- Wilens T, Zulauf C, Ryland D, Carrellas N, Catalina-Wellington I. Prescription medication misuse among opioid dependent patients seeking inpatient detoxification. The American journal on addictions/American Academy of Psychiatrists in Alcoholism and Addictions. 2015;24:173–177.
- Hakkinen M, Vuori E, Kalso E, Gergov M, Ojanpera I. Profiles of pregabalin and gabapentin abuse by postmortem toxicology. Forensic science international. 2014;241:1–6.
- Hakkinen M, Vuori E, Kalso E, Gergov M, Ojanpera I. Profiles of pregabalin and gabapentin abuse by postmortem toxicology. Forensic science international. 2014;241:1–6.
- Smith BH, Higgins C, Baldacchino A, Kidd B, Bannister J. Substance misuse of gabapentin. The British journal of general practice: the journal of the Royal College of General Practitioners. 2012;62:406–407.
- Schifano F, D’Offizi S, Piccione M, Corazza O, Deluca P, Davey Z, et al. Is there a recreational misuse potential for pregabalin? Analysis of anecdotal online reports in comparison with related gabapentin and clonazepam data. Psychotherapy and psychosomatics. 2011;80:118–122.
- Evoy, K.E., Peckham, A.M., Covvey, J.R. and Tidgewell, K.J. (2021), Gabapentinoid Pharmacology in the Context of Emerging Misuse Liability. The Journal of Clinical Pharmacology, 61: S89-S99.
- Connecticut Department of Consumer Protection. (n.d.). Pharmacist Information. Retrieved February 25, 2023, from https://portal.ct.gov/DCP/Prescription-Monitoring-Program/Pharmacist-Information
- District of Columbia Department of Health. (2019). Chapter 103: Prescription Drug Monitoring Program. Retrieved from https://dchealth.dc.gov/sites/default/files/dc/sites/doh/publication/attachments/Chapter%20103%20PDMP.6.7.19.pdf
- Indiana Professional Licensing Agency. (n.d.). Frequently asked questions. Retrieved February 25, 2023, from https://www.in.gov/pla/inspect/faqs/#Q3
- Indiana Professional Licensing Agency. (n.d.). News and important announcements. Retrieved February 25, 2023, from https://www.in.gov/pla/inspect/news-and-important-announcements/
- Indiana Professional Licensing Agency. (n.d.). Frequently asked questions. Retrieved February 25, 2023, from https://www.in.gov/pla/inspect/faqs/#Q3
- Kansas Department of Health and Environment. (2020). 2020 legislative report: K-TRACS. Retrieved February 25, 2023, from https://pharmacy.ks.gov/docs/librariesprovider10/ktracs/reports/2020-legislative-report-k-tracs.pdf?sfvrsn=13ddaa01_4
- Kansas Department of Health and Environment. (n.d.). K-TRACS: Pharmacists reporting to K-TRACS. Retrieved February 25, 2023, from https://pharmacy.ks.gov/k-tracs/pharmacists/reporting-to-k-tracs
- Massachusetts Department of Public Health. (2017, September 12). 105 CMR 700: Prescription monitoring program. Retrieved February 25, 2023, from https://www.mass.gov/files/documents/2017/09/12/105cmr700.pdf
- Massachusetts Department of Public Health. (n.d.). Pharmacy reporting and data submission. Retrieved February 25, 2023, from https://www.mass.gov/service-details/pharmacy-reporting-and-data-submission
- Minnesota Revisor of Statutes. (n.d.). 152.126. Prescription monitoring program. Retrieved February 25, 2023, from https://www.revisor.mn.gov/statutes/cite/152.126
- Minnesota Board of Pharmacy. (n.d.). Submitters reporting. Retrieved February 25, 2023, from https://mn.gov/boards/pharmacy-pmp/submitters/reporting/
- Nebraska Department of Health and Human Services. (n.d.). Nebraska prescription drug monitoring program (PDMP) SFTP submitter guide. Retrieved February 25, 2023, from https://dhhs.ne.gov/DOP%20document%20library/Nebraska%20PDMP%20SFTP%20Submitter%20Guide.pdf
- New Jersey Division of Consumer Affairs. (n.d.). Prescription Monitoring Program (PMP) regulations. Retrieved February 25, 2023, from https://www.njconsumeraffairs.gov/regulations/Chapter-45A-Subchapter-35-Prescription-Monitoring-Program.pdf
- Ohio Board of Pharmacy. (n.d.). Update on gabapentin in Ohio. Retrieved February 25, 2023, from https://www.pharmacy.ohio.gov/documents/pubs/newsletter/2019/update%20on%20gabapentin%20in%20ohio.pdf
- Ohio Administrative Code. (n.d.). 4729:8-2-02. Prescription monitoring program. Retrieved February 25, 2023, from https://codes.ohio.gov/ohio-administrative-code/rule-4729:8-2-02
- Oregon Health Authority. (n.d.). Prescription drug monitoring program (PDMP). Retrieved February 25, 2023, from https://www.oregon.gov/oha/ph/preventionwellness/safeliving/pdmp/pages/index.aspx#:~:text=As%20of%20January%201%2C%202020,for%20each%20covered%20substance%20dispensed.
- Utah Admin. Code R156-37f-203 (2021). https://www.law.cornell.edu/regulations/utah/Utah-Admin-Code-R156-37f-203
- Utah Office of Administrative Rules. (2019, November 1). DAR file no. 44120. https://rules.utah.gov/publicat/bulletin/2019/20191101/44120.htm
- Wyoming State Board of Pharmacy. (2012). Board of Pharmacy Wyoming Controlled Substances Act Rules and Regulations. https://wyoleg.gov/arules/2012/rules/ARR17-012.pdf
- Illinois General Assembly. (n.d.). Illinois Compiled Statutes: 720 ILCS 570/316. Retrieved from https://www.ilga.gov/legislation/ilcs/fulltext.asp?DocName=072005700K316
- Alabama Legislature. (n.d.). Section 20-2-213 Reporting requirements. Code of Alabama 1975. Retrieved from http://alisondb.legislature.state.al.us/alison/CodeOfAlabama/1975/20-2-213.htm
- Cabinet for Health and Family Services. (2022). Kentucky Administrative Regulations Chapter 55. Retrieved from https://www.chfs.ky.gov/agencies/os/oig/dai/deppb/Documents/KentuckyAdministrativeRegulationsChapter55.pdf
- Kentucky Legislature. (n.d.). KRS 218A.202(3)(a) (b) and (c)
- Michigan Department of Licensing and Regulatory Affairs. (n.d.). Data Submitters. Retrieved from https://www.michigan.gov/lara/bureau-list/bpl/health/maps/data-submitters
- North Dakota Board of Pharmacy. (n.d.). Prescription Drug Monitoring Program Frequently Asked Questions. Retrieved from https://www.nodakpharmacy.com/PDMP-faq.asp
- Tennessee Department of Health. (n.d.). FAQ’s Controlled Substance Monitoring Database (CSMD) and Prescription Safety Act. Retrieved from https://www.tn.gov/health/health-program-areas/health-professional-boards/csmd-board/csmd-board/faq.html
- Virginia Law. (n.d.). § 54.1-2521. Reporting requirements. Retrieved from https://law.lis.virginia.gov/vacode/title54.1/chapter25.2/section54.1-2521/
- Virginia Law. (n.d.). § 54.1-2522. Reporting exemptions. Retrieved from https://law.lis.virginia.gov/vacode/title54.1/chapter25.2/section54.1-2522/
- State of West Virginia Board of Pharmacy. (2019). West Virginia Controlled Substance Automated Prescription Program Procedures and Policies. National Association of State Controlled Substances Authorities. Retrieved from https://www.nascsa.org/documents/dispenserGuides/WestVirginia-V42.pdf
- Oregon Health Authority. (n.d.). Oregon PDMP Data Submission Dispenser Guide. [PDF file]. Retrieved February 25, 2023, from https://www.oregon.gov/oha/PH/PREVENTIONWELLNESS/SAFELIVING/PDMP/Documents/Oregon_PDMP_Data_Submission_Dispenser_Guide.pdf